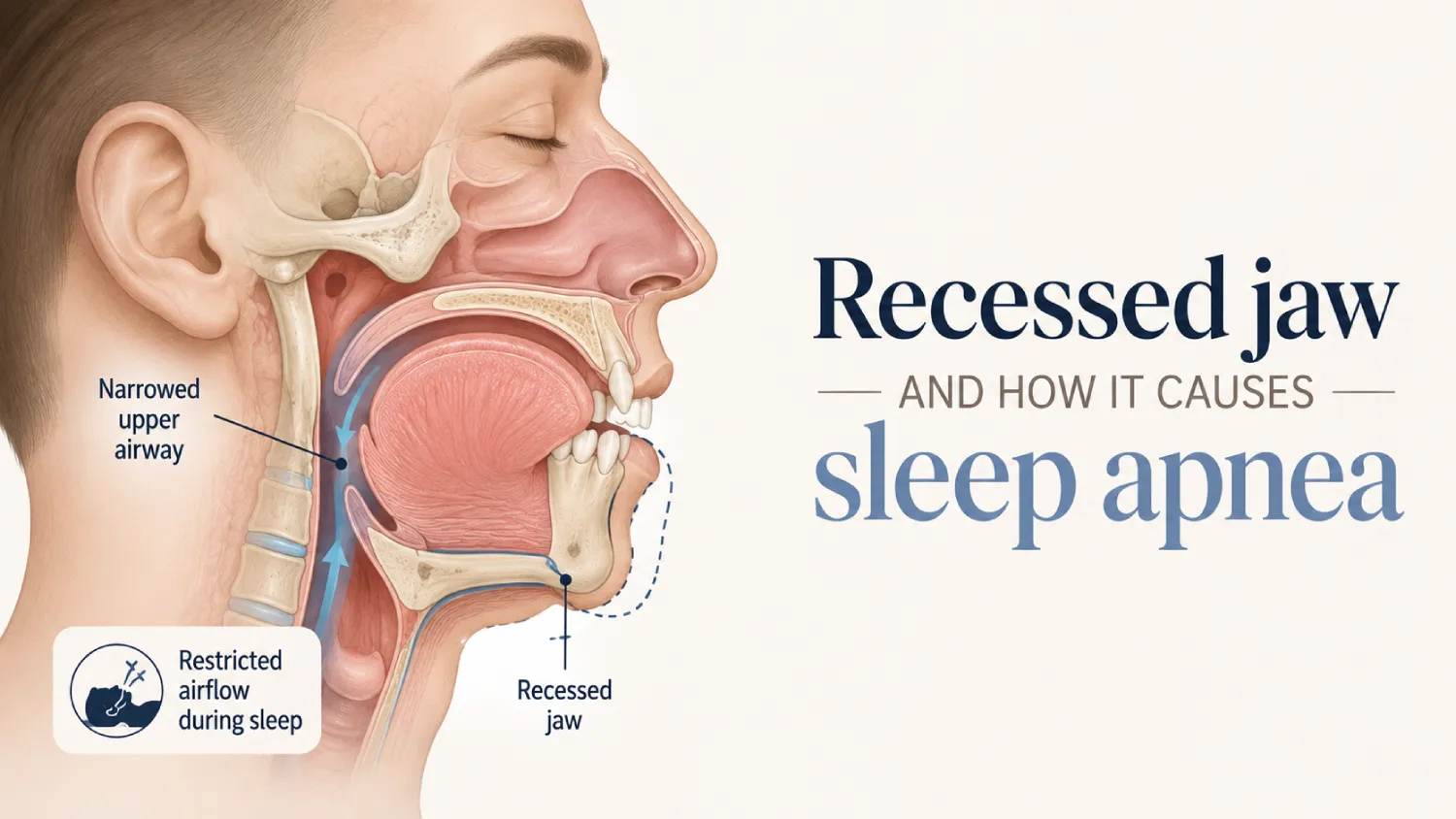
A 2026 study highlighted the rural sleep apnea diagnosis gap. Here is the new access model that brings diagnosis to patients where they live.
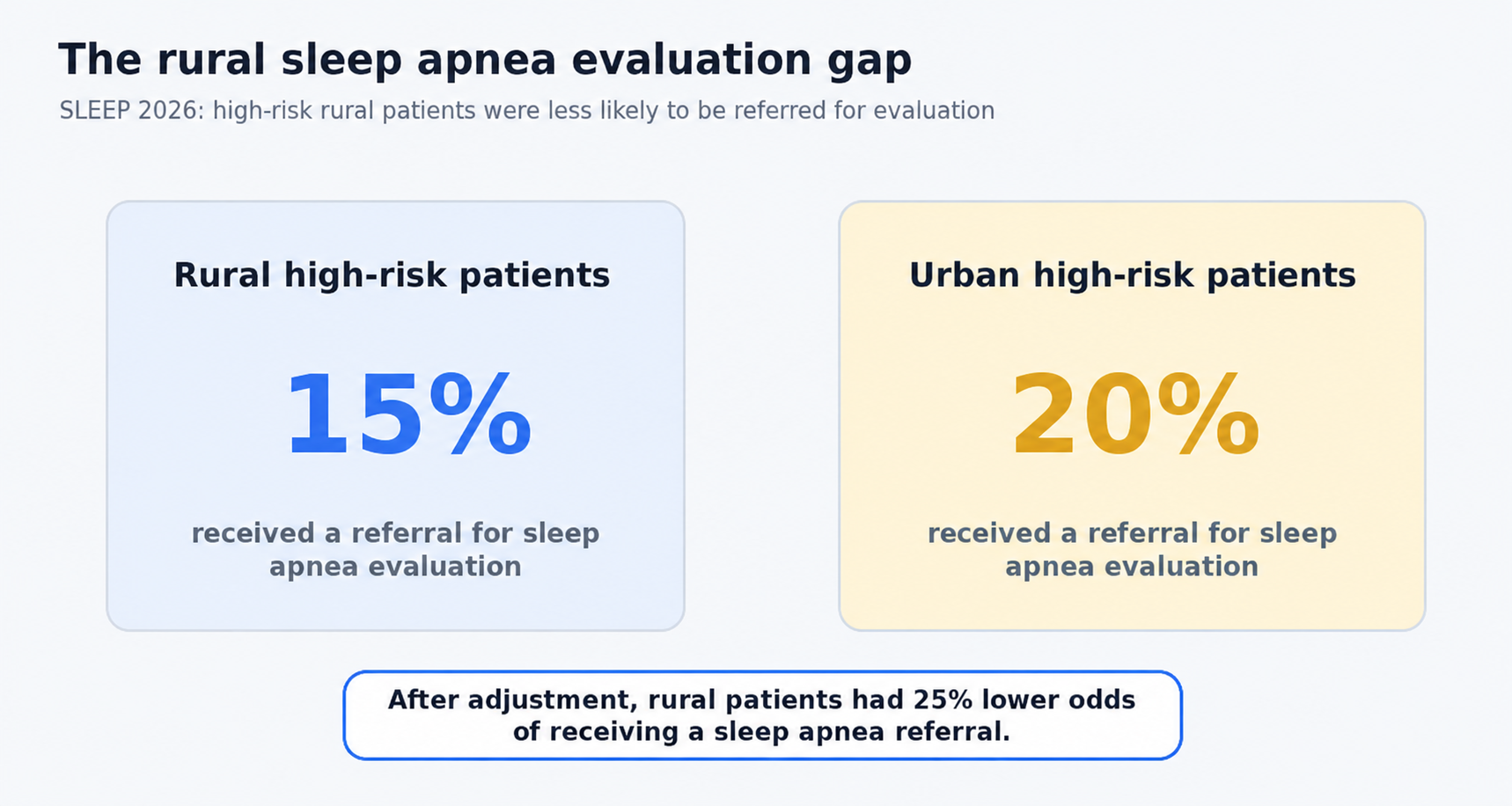
A study presented at SLEEP 2026 found that high-risk rural primary-care patients were less likely than urban patients to be referred for sleep apnea evaluation, the step that can lead to a sleep apnea diagnosis. Among 25,917 high-risk patients, only 15% of rural patients received a referral for sleep apnea evaluation compared with 20% of urban patients. After adjustment, rural patients had 25% lower odds of receiving a sleep apnea referral.
Read the numbers slowly. A patient living in a rural area, with the same clinical risk as a patient living in a city, has historically been less likely to be offered the evaluation that could lead to a sleep apnea diagnosis. Same disease. Same risk. Different zip code. Different pathway.
This is the story rural healthcare has been working to change for years. And now, for the first time, the pieces exist to make sleep apnea diagnosis access less dependent on geography.
Sleep care has historically been concentrated in cities
Sleep medicine, as a clinical specialty, grew up around hospital-based sleep labs and metropolitan specialty networks. The trained sleep physicians, accredited sleep labs, and multidisciplinary care teams are often clustered where population density supports the infrastructure.
For a patient in a city, a sleep referral may lead to an appointment within weeks. For a patient in a rural county, the same referral has traditionally meant a longer drive, a longer wait, and a heavier total cost.
The disease burden does not concentrate only in cities. The infrastructure that produces sleep apnea evaluation and diagnosis often does.
The SLEEP 2026 data gives a clear picture of where rural sleep care currently sits. The patients are present. The risk is present. The gap is in how consistently the diagnostic pathway reaches them.
The study authors pointed to rural-specific structural barriers that can make referral and evaluation harder. Those barriers include distance from sleep centers, limited availability of sleep medicine clinicians, and socioeconomic factors that make time, transportation, and out-of-pocket costs more difficult to absorb.
These barriers are not individual failures. They are structural realities of how sleep apnea evaluation has historically been distributed. They are also exactly the barriers newer access models are positioned to address.
Three capabilities have matured at the same time, and together they make rural sleep care look fundamentally different from how it has looked for the last two decades.
Each piece has existed in some form before. The new access model is the combination. Together, they make the sleep apnea diagnostic pathway more available to patients where they live.
The first step in the new access model is identification, and this is where rural settings have historically faced the widest gap. If patients at high risk are never identified or never routed into evaluation, the diagnosis never happens.
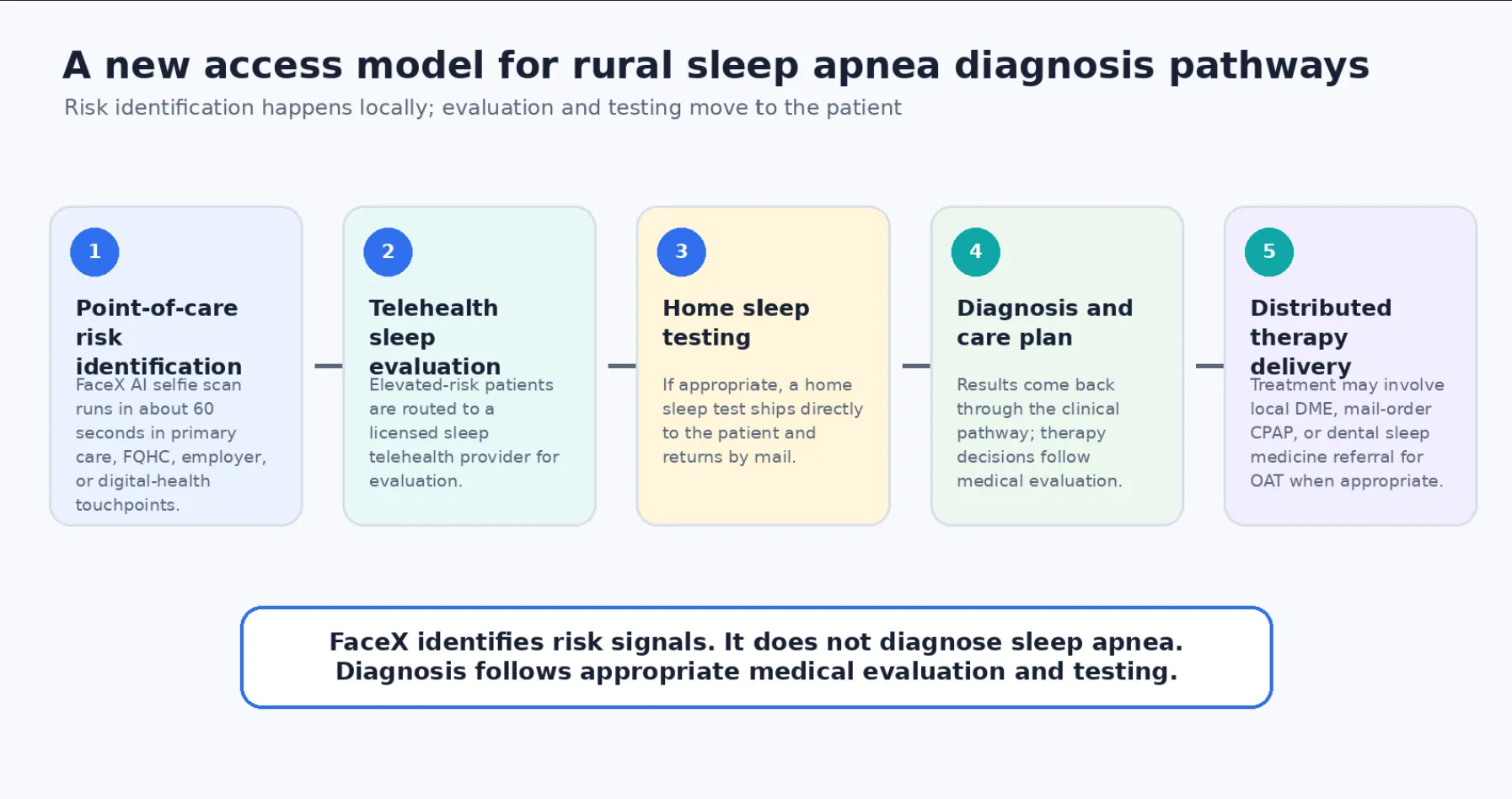
Soliish’s FaceX AI selfie scan for obstructive sleep apnea analyzes facial markers associated with sleep apnea risk in about 60 seconds. The screening runs on a smartphone or tablet. It can be deployed in a rural primary-care office during a routine visit, in a federally qualified health center, in an employer wellness program serving a rural workforce, or as part of a digital health platform that reaches patients directly.
FaceX does not diagnose obstructive sleep apnea. It identifies risk signals that can help route elevated-risk patients into an appropriate diagnostic pathway.
In practical terms, the identification step no longer has to wait for a specialist visit. A patient in a rural county can be screened during the visit they were already attending, with a documented risk signal produced at the point of care. The patient does not travel. The clinician does not need specialty sleep-medicine training. The identification happens where the patient already is.
For rural primary care, that turns the front end of the diagnostic pathway from an aspirational referral into an operational reality.
Identification only matters if the patient can reach evaluation. This is where sleep telehealth completes the access model.
Soliish routes elevated-risk patients to Arima Health, a national sleep telehealth provider, for diagnostic evaluation. The patient completes the consultation from home. If appropriate, the home sleep test ships directly to the patient and is returned by mail. Results come back through the telehealth pathway, and treatment decisions are made through the appropriate clinical process.
The rural patient does not have to travel to a sleep clinic for the initial evaluation pathway. Clinician availability is addressed through a broader telehealth network rather than only the closest geographic specialist.
This is not a workaround. It is the access model rural sleep care has been waiting for.
The combination is what closes the access gap.
A rural primary-care office that runs Soliish’s FaceX AI scan at the front end of the visit can produce documented sleep apnea risk identification for patients who may otherwise never enter the pathway. Patients flagged at elevated risk can be routed to Arima for telehealth evaluation. Patients who receive a sleep apnea diagnosis can then enter the treatment pathway their physician recommends, which may include local DME for CPAP, mail-order CPAP, or referral to dental sleep medicine providers for oral appliance therapy when appropriate.
The rural patient does not need the same local infrastructure as an urban patient to receive a complete pathway from risk identification to treatment decisions. The journey can be executed through local screening, telehealth diagnostics, home sleep testing, and distributed therapy delivery.
Geography stops being the deciding factor. The diagnostic pathway becomes available closer to where the patient lives.
Soliish is not a complete rural sleep-care solution by itself. The model requires multiple pieces working together.
What Soliish provides is the identification layer: the screening that produces a documented risk signal at the point of care, regardless of the patient’s distance from a sleep specialist. The platform partners with Arima Health for the telehealth diagnostic pathway, with DME providers for therapy fulfillment, and with dental sleep medicine practices for oral appliance therapy. The full pathway is collaborative, with each partner contributing the piece they are best positioned to deliver.
The identification layer is where rural access begins. A patient who is identified can be routed. A patient who is routed can be evaluated. A patient who is evaluated can receive a sleep apnea diagnosis. A patient who is diagnosed can be treated.
For rural primary-care offices, federally qualified health centers, employers with rural workforces, and healthcare partners that touch rural populations, the opportunity is to build identification into the touchpoints they already have with patients. Once identification is happening consistently, the rest of the pathway has somewhere to start.
In a rural primary-care office running this model, screening adds about a minute to the patient visit. The patient completes the selfie scan themselves on a smartphone or tablet. The result lands in the patient record. Patients flagged at elevated risk are offered a telehealth sleep consultation, which they complete from home. The home sleep test arrives by mail. The diagnostic result comes back through the telehealth pathway.
Within weeks, a rural patient who might historically have remained undiagnosed can have a clinical answer to symptoms they may have carried for years. The local primary-care physician has diagnostic confirmation to support ongoing care coordination. The therapy pathway is supported by whichever local or distributed partner makes sense for the patient.
The access gap closes one patient at a time, through a model that respects the realities of rural healthcare and adds the technology layer that completes the pathway.
Distance should not decide who gets access to a sleep apnea diagnosis. The opportunity is for rural primary care, federally qualified health centers, employers with rural workforces, and digital health platforms to build identification into the touchpoints they already have.


Rural patients may face barriers such as distance from sleep centers, limited sleep-specialist availability, transportation challenges, time costs, and other socioeconomic factors.
A clinician may recommend home sleep apnea testing for some patients. Whether home testing or in-lab testing is appropriate depends on the patient’s symptoms, risk factors, and medical history.
No. FaceX identifies risk signals associated with obstructive sleep apnea. Diagnosis requires appropriate clinical evaluation and testing.
Rural primary care can help identify elevated-risk patients earlier and route them into telehealth evaluation or other appropriate diagnostic pathways.