

The ADA has formally encouraged dentists to screen for sleep-related breathing disorders. Here is what the 2019 policy says, and what acting on it looks like.
The American Dental Association gives dentistry a clear role in sleep-health conversations. In its policy statement on sleep-related breathing disorders, the ADA encourages dentists to screen patients for risk as part of a comprehensive medical and dental history, refer at-risk patients to appropriate physicians for diagnosis, and provide oral appliance therapy when it is prescribed and clinically appropriate.
That guidance is important, but it does not turn itself into a working program. For dental practices and DSOs, the real challenge is building a responsible workflow that teams can use consistently without adding meaningful chair time to an already busy visit.
The question is no longer whether sleep health belongs in the dental conversation. The question is how to act on the ADA’s guidance without overstepping clinical boundaries, overwhelming the team, taking up too much chair time, or losing patients between screening and evaluation.
What does the ADA say about dentists and sleep apnea?
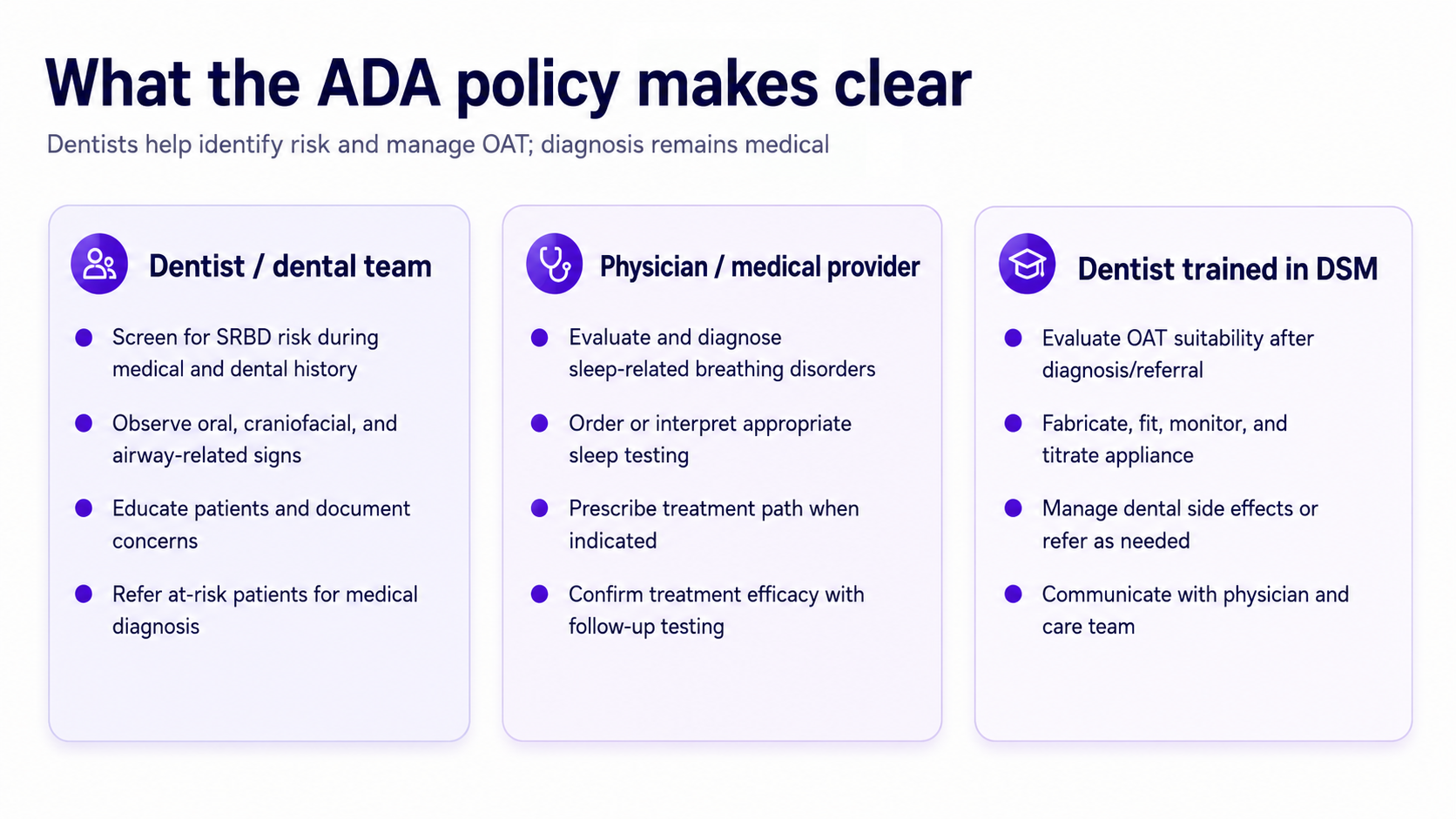
The ADA policy says dentists are well positioned to identify patients who may be at greater risk for sleep-related breathing disorders, including obstructive sleep apnea. It encourages dentists to screen patients as part of a comprehensive medical and dental history and to refer patients, as needed, to appropriate physicians for proper diagnosis.
The policy also recognizes the dentist’s role in oral appliance therapy. When a physician diagnoses obstructive sleep apnea and recommends oral appliance therapy through referral, a dentist should evaluate whether the patient is appropriate for a suitable oral appliance, fabricate the appliance when appropriate, monitor effectiveness, and titrate the appliance as needed.
That distinction matters. Dentists can identify risk, educate patients, support referral, and manage the dental side of oral appliance therapy. Diagnosis remains the role of the appropriate medical provider.
The ADA policy encourages dentists to screen patients for sleep-related breathing disorders. It does not say every dentist is required to screen every patient.
Even so, the policy makes sleep-related breathing disorders part of the broader conversation around comprehensive dental care. Dentists routinely review medical history, observe oral and craniofacial anatomy, and hear patient concerns such as snoring, fatigue, dry mouth, morning headaches, and witnessed breathing pauses.
The practical question for a practice is not only “Can we talk about this?” It is “How do we talk about this responsibly and consistently?”
The ADA policy points to symptoms and risk factors that may appear in a patient’s history or during dental care. Examples include:
Some of these are reported by the patient. Others may be visible during a routine dental exam. Dental teams regularly observe craniofacial structures, oral anatomy, tongue position, palate shape, bite patterns, and airway-related anatomy.
A dentist should not diagnose sleep apnea from these observations. But the dental team can notice patterns, educate patients, document concerns, and guide appropriate evaluation pathways.
The ADA recognizes oral appliance therapy as part of dentistry’s role in sleep-related breathing disorder care. Oral appliance therapy may be appropriate for mild to moderate sleep apnea and for some patients with severe sleep apnea who cannot tolerate CPAP, when medically diagnosed and appropriately referred.
The dentist’s role may include evaluating oral structures, fabricating or fitting the appliance, titrating it, monitoring effectiveness, managing dental side effects, and communicating with the referring physician.
This is not a replacement for medical care. It is a coordinated model: the physician diagnoses and prescribes, and the dentist provides and manages the appliance when appropriate.
Acting on the ADA policy requires more than adding a question about snoring to the intake form. A practice needs a workflow that is clear, repeatable, and clinically responsible.
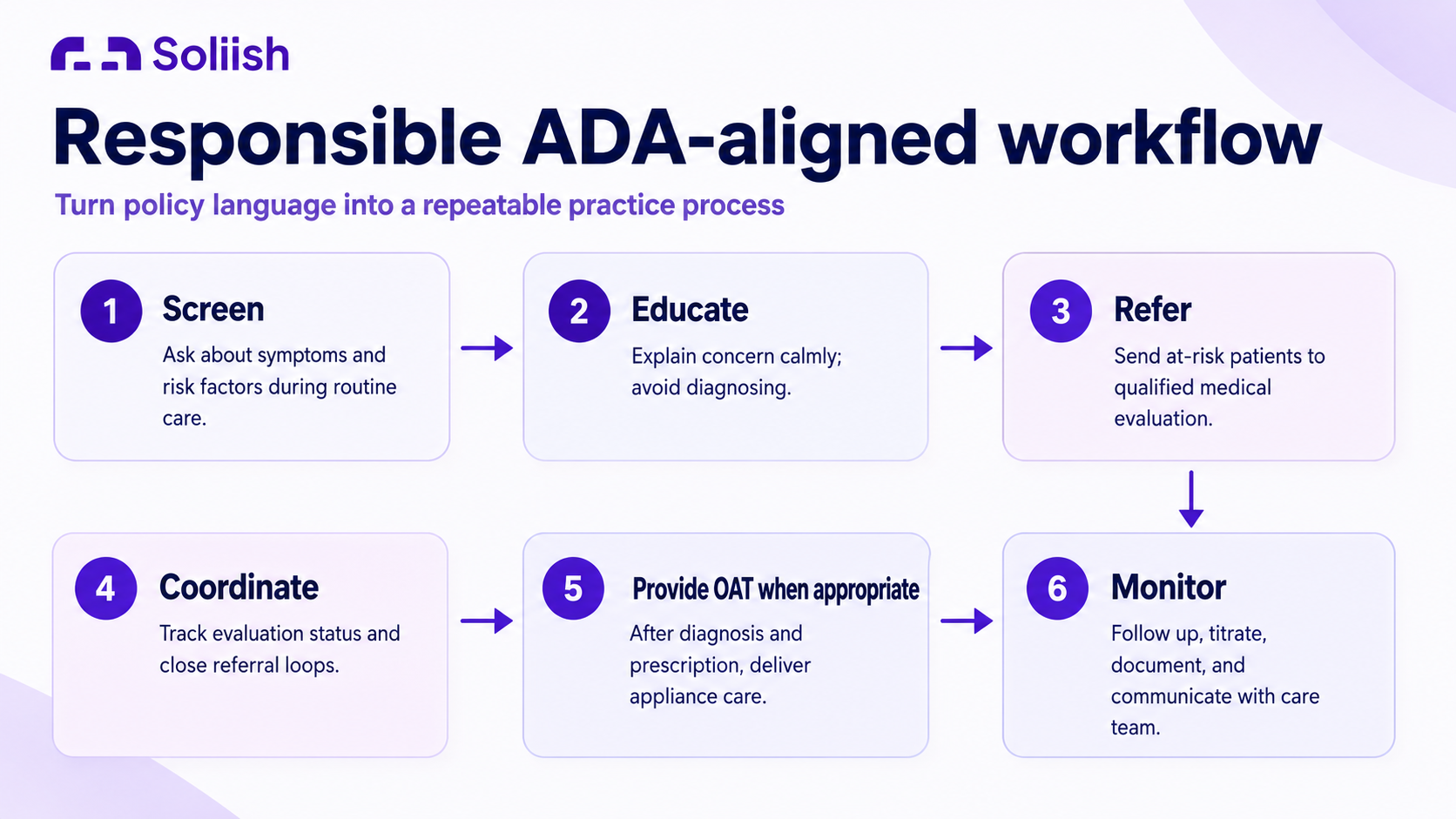
1. A consistent screening process
The practice needs a standard way to start sleep-health conversations. This may include digital intake questions, chairside discussion, facial analysis, or a structured workflow that combines symptom history with anatomy-related observations.
2. A clear referral pathway
Screening has limited value if there is no next step. Practices need a relationship with sleep providers, local physicians, tele-sleep partners, or other qualified medical teams who can evaluate patients and order appropriate testing.
3. Team training
The whole team needs to understand the workflow. Hygienists may introduce the conversation. Dentists may explain the relevance of oral and craniofacial signs. Front desk teams may help with referral steps or follow-up communication.
4. Oral appliance therapy infrastructure
If the practice provides oral appliance therapy, it needs dental sleep medicine training, medical documentation workflows, lab relationships, fitting and titration protocols, follow-up schedules, side-effect monitoring, billing support, and communication with sleep physicians.
5. Tracking and visibility
A sleep-health program needs follow-through. Practices should be able to see who was screened, who was identified as at risk, who accepted referral, who completed evaluation, who returned for oral appliance therapy after medical evaluation, and where patients drop off.
6. Chair-time-conscious tools
For adoption to last, the workflow has to be easy to use during real appointments. Tools like Soliish can help by moving part of the education and risk-engagement process into a guided selfie or face scan experience. That gives the dental team a structured way to discuss orofacial and airway health clues without taking up a lot of additional chair time.
For a single dental practice, an ADA-aligned sleep-health workflow can start small. The practice may begin with digital intake questions, team training, and a referral relationship with a sleep provider. Over time, it can add more structured documentation, patient education, and oral appliance therapy support if that fits the practice model.
The goal is not to overwhelm the team. The goal is to make sleep-health conversations easier to start and easier to route. A patient mentions snoring. The hygienist knows what to ask next. The dentist can explain what they see. The patient understands why evaluation may matter. The referral pathway is already in place.
That is how a policy becomes a workflow.

For DSOs, the challenge is scale. One motivated dentist can start a sleep-health conversation. A DSO needs a consistent process across locations, teams, and patient populations.
That requires standard intake workflows, consistent patient education, clear provider training, referral coordination, centralized visibility, location-level reporting, support for implementation and billing, and defined pathways for oral appliance therapy when appropriate.
Once the workflow is standardized, each location does not have to reinvent it. New practices can adopt the same baseline process. Leaders can see where referrals are moving, where patients are dropping off, and where additional training may be needed.

Facial analysis and a selfie-based face scan may help identify visible facial, orofacial, and airway-related traits associated with elevated sleep apnea risk. This does not diagnose sleep apnea, but it can support patient education, visual engagement, and appropriate evaluation pathways.
Many patients do not connect snoring, fatigue, dry mouth, morning headaches, jaw structure, or airway health with sleep. A visual engagement tool can make the conversation more concrete, easier to understand, and faster to introduce during a routine visit.
Used responsibly, facial analysis can support the front end of the workflow: it can help start a conversation, document risk signals, and guide patients toward appropriate medical evaluation without requiring the dentist to spend extra chair time explaining every risk factor from scratch. It should not be positioned as a diagnostic substitute.
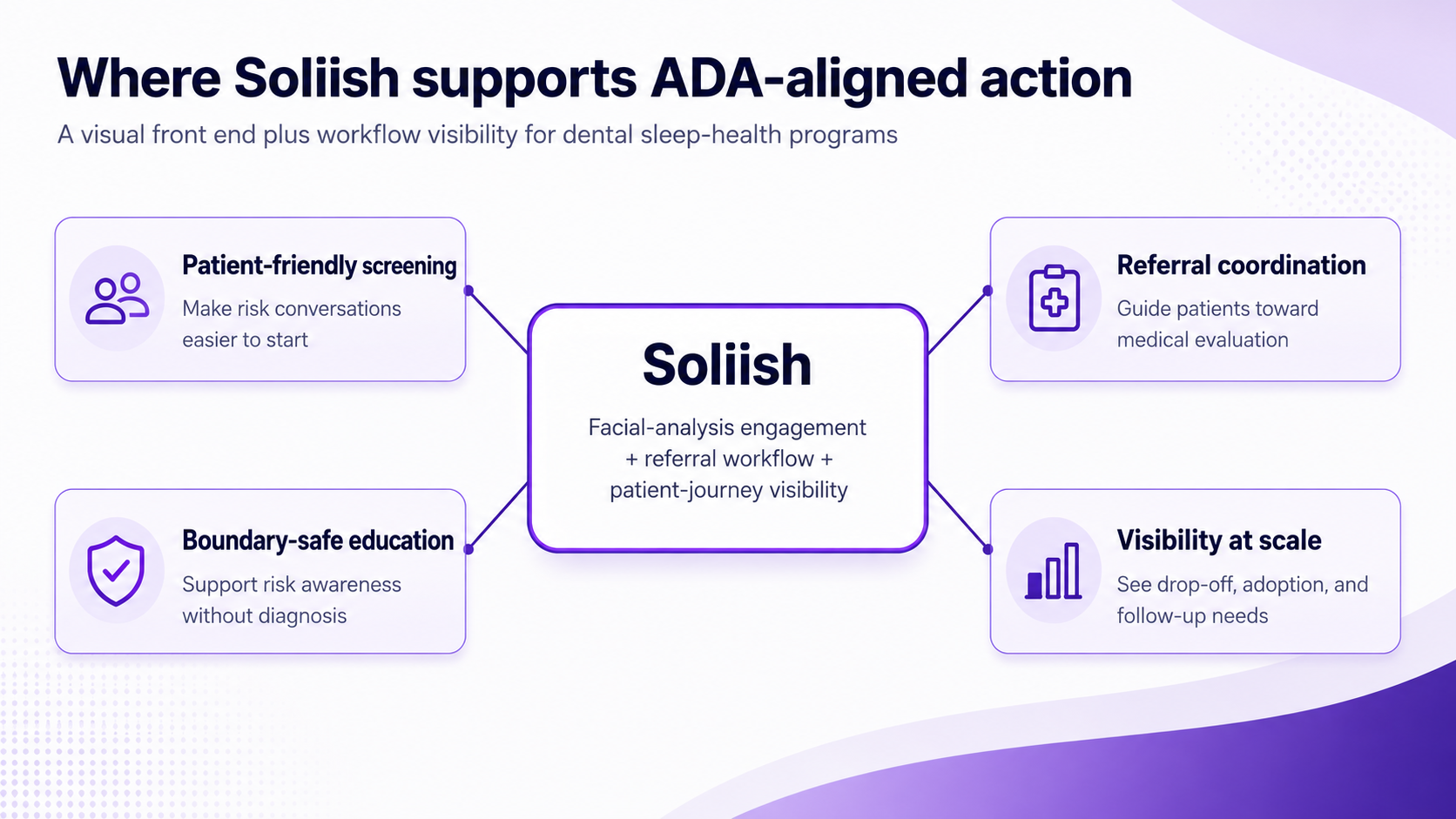
Soliish is a facial-analysis-driven engagement and workflow platform for dental sleep-health programs. For dental practices and DSOs, it supports the operational side of ADA-aligned care.
Soliish helps teams start sleep-health conversations in a patient-friendly way, use facial analysis as a visual education tool, standardize workflows across teams and locations, improve referral visibility, support coordinated care pathways, reduce referral leakage, and improve visibility across the patient journey.
This matters because many dental sleep programs do not fail because dentists lack interest. They fail because the workflow is hard to run. Screening is inconsistent. Referrals are manual. Follow-up is unclear. Teams are unsure what to say. Leaders cannot see what is happening across the patient journey.
Soliish helps bring structure to that process.
The ADA’s sleep-related breathing disorders policy gives dentistry a clear role in sleep health. It encourages dentists to identify patients who may be at risk, support sleep-health conversations, and refer patients to appropriate physicians for diagnosis. It also recognizes the dentist’s role in oral appliance therapy when prescribed by a physician.
But the policy does not implement itself. Practices and DSOs need workflows, training, referral pathways, documentation, and visibility.
Soliish supports that operational gap. As a facial-analysis-driven engagement and workflow platform, Soliish helps dental teams bring sleep-health conversations into routine care in a more consistent, visual, and scalable way.
See how Soliish helps practices add ADA-aligned sleep-health workflows without adding a heavy chair-time burden.


The ADA encourages dentists to screen patients for sleep-related breathing disorders, including obstructive sleep apnea, as part of a comprehensive medical and dental history. At-risk patients should be referred to appropriate physicians for diagnosis.
No. The ADA encourages screening but does not require every dentist to screen every patient. The policy supports screening as an appropriate role within dental practice.
No. Dentists do not diagnose sleep apnea. Diagnosis requires appropriate medical evaluation and, when indicated, a sleep study interpreted by qualified medical providers.
Yes, dentists trained in dental sleep medicine can provide oral appliance therapy when it is prescribed by a physician and appropriate for the patient.
Dentists may ask about snoring, daytime sleepiness, witnessed breathing pauses, choking or gasping during sleep, dry mouth, morning headaches, and other sleep-health concerns as part of a broader health history.
Dentists may observe craniofacial and airway-related anatomy, including jaw position, tongue size, palate shape, bite patterns, and other oral structures that may be relevant to sleep-health conversations.
Facial analysis may help identify facial traits associated with elevated sleep apnea risk. It supports patient education and engagement, but it does not diagnose sleep apnea or replace a sleep study.
Soliish supports ADA-aligned sleep-health workflows by combining facial-analysis-driven patient engagement with care coordination and operational infrastructure. It helps practices improve visibility across the patient journey and build scalable dental sleep workflows.


